Fertilization, Menopause, the Events of Pregnancy, Labour and Birth.
Hello, readers. Thanks for all the encouragement and motivation. Today, I will continue from where I stopped on WHAT IS SEX FOR? #2
Talking about menstrual cycle and pregnancy. In the events of pregnancy, If the egg cell is fertilised, the menstrual cycle is interrupted and the female’s body changes in response to the events of pregnancy.
Fertilization is a complex sequence of events that begins when the sperm reaches the egg cell (oocyte). The secondary oocyte is surrounded by several layers of follicle cells, the corona radiata, and a layer of glycoprotein, the zona pellucida. Before a sperm can penetrate the layers surrounding the oocyte, it undergoes a process called capacitation. The actual mechanism is poorly understood, but it seems to set off the acrosome reaction, which allows the sperm head to enter the oocyte. The acrosome is a bag of digestive enzymes on the tip of the sperm head. During the acrosome reaction, the bag splits, releasing the enzymes, which digest a pathway through any remaining follicle cells and the zona pellucida.

As soon as the outer membrane of the first sperm penetrates the cell surface membrane of the oocyte, a rapid reaction occurs. Many cortical granules fuse with the zona pellucida, forming a fertilization membrane. This reaction starts at the point of entry of sperm head and spreads rapidly over the surface of the oocyte, preventing entry of other sperm. So, only one sperm enters the diploid secondary oocyte, even though many reach it at the same time. Entry of the sperm nucleus triggers the completion of meiosis II in the female nucleus leading to the formation of the second polar body and a haploid mature ovum.
Almost immediately afterwards, a spindle forms and the paternal and maternal chromosomes come together, forming a diploid zygote. Within 12 hours, the first mitotic division takes place. Cell division is now rapid, forming a bundle of cells called a morula (Latin for the blackberry it resembles). As divisions continue, this becomes a blastocyst and moves slowly along the Fallopian tube through the action of cilia, which create a steady current of fluid towards the uterus.
It takes around 6 or 7 days to complete the journey down the Fallopian tube. When the blastocyst arrives at the uterus on day 21 of the cycle, the lining must be in just the right condition to accept it. For a successful pregnancy there must be exact timing between the preparation of the endometrium and the development of the embryo.
Implantation
Pregnancy begins not with fertilization but when the blastocyst implants in the wall of the uterus. This happens about a week after fertilisation and is not always successfully completed. Many women trying to conceive may have a ‘near miss’, when an egg is fertilised but fails to implant.
Implantation begins when the blastocyst makes contact with the endometrium, usually on the back wall. The outer layer of the blastocyst, the trophoblast, causes an inflammatory-type response (normally a response to damage) and this causes an outgrowth of the endometrium at this point. The placenta develops where the trophoblast and the endometrium interact.
If implantation is successful, the embryo begins to secrete human chorionic gonadotrophin (hCG). This hormone forces the coгpus luteum in the ovary to continue to secrete progesterone, thereby maintaining the endometrium and inhibiting FSH production.
The chorion, one of the membranes that later grows and surrounds the embryo, develops villi (projections) that burrow into the endometrium. These are thought to break down the mother’s blood vessels, causing the chorionic villi to become bathed in maternal blood.
THE MENOPAUSE AND HORMONE REPLACEMENT THERAPY
The menopause is a natural event that occurs when the ovaries stop working. For most women, this happens between the ages of 45 and 54. This time is often difficult and traumatic. The lowered levels of oestrogen and progesterone are directly responsible for the unpleasant symptoms of the menopause:
- Circulatory problems such as hot flushes and night sweats.
- Psychological problems, such as depression, anxiety and insomnia.
- Skeletal problems. Oestrogen inhibits reabsorption of bone, and after the menopause, bone loss can be as great as 7 per cent per year. This condition, osteoporosis, affects the spongy bone particularly and the sufferer is more likely to break a bone.
- Oestrogen is also thought to give women some protection against some types of heart disease. Women below menopausal age are less likely than men to have heart disease, but afterwards they catch up.
Hormone replacement therapy can help to reverse many of these symptoms and effects. The basic idea behind HRT is simple: to restore hormone levels to those of the early follicular phase of the menstrual cycle using tablets, implants or transdermal patches.
THE PLACENTA
The placenta is a temporary organ that allows the blood systems of the fetus and the mother to come into close contact, without actually mixing. The placenta allows nutrients and oxygen to pass to the fetus from the mother, and allows metabolic waste back into the mother’s blood. It is an organ adapted to maximize the exchange of materials, so, as you would expect, it has a large surface area provided by the chorionic villi. A close look at the cells of the villi shows that the membranes are folded into microvilli and also contain many mitochondria: these two features maximize the processes of diffusion and active transport. There are many small vesicles in the cells of the villi, suggesting that substances are being absorbed by pinocytosis.
The placenta is an important endocrine organ. It secretes the hormones that maintain pregnancy, taking over from the corpus luteum at about 12 weeks. The placenta secretes progesterone (which maintains the endometrium), oestrogen (which inhibits the ovulatory cycle), human chorionic gonadotrophin and human placental lactogen (which stimulates the development of the mammary glands).

INFERTILITY AND ITS TREATMENT
Nine out of ten couples that use no contraception and actively try to conceive are successful within a year. But one in ten couples may face the distressing problem of infertility. Many are ‘sub-fertile’ rather than infertile, and can be helped by the various methods described here. However, for a few, nothing works. Remaining childless when you desperately want a family can be very traumatic and couples may need help and counselling to come to terms with their inability to reproduce.
There are several possible causes of infertility and there are now many treatments, as a result of a great deal of research over the past 20 years. This has not been without controversy but it has helped many couples who would otherwise have been unable to conceive.
Causes of infertility
Doctors accept that a couple may need infertility treatment if they have been trying to conceive for at least a year without any success. The first objective is to establish whether either partner has an obvious problem that is preventing conception. Couples are also recommended to try to establish when exactly the woman ovulates during the month using temperature charts and looking for changes in the consistency of vaginal mucus. Having sex at the most fertile time could be all that is needed. However, some couples still fail to conceive.
Female infertility may be caused by:
- Blocked Fallopian tubes.
- Altered hormone levels leading to a failure to ovulate or implant. Failure to ovulate, known as anovulatory infertility, is usually due to a failure to secrete the right balance of hormones.
- Cervical mucus that halts, repels or kills sperm.
Male infertility may be caused by:
- A low sperm count. Samples that are found to have fewer than 20 million sperm per cm3 are said to be abnormally low.
- Production of large numbers of abnormal sperm (more than four per cent).
- Production of antibodies that make the sperm stick together.
Ovulation induction
A woman sometimes does not ovulate because the balance of hormones in her body is abnormal. To restore the hormone levels and initiate follicle development and ovulation, she can have treatment with artificial gonadotrophins or drugs that stimulate the natural secretion of gonadotrophins. One such drug, clomiphene, works by increasing FSH secretion.
After such treatment, the response of the ovaries can be followed by ultrasound, which shows how many follicles are developing in each ovary. A follicle is considered to be ready for ovulation when it reaches 17 mm in diameter. The endometrium is also checked – it should be at least 8 mm thick at this time. When a ripe follicle is detected, ovulation can be stimulated artificially by injecting human chorionic gonadotrophin (hCG), a hormone that has a similar effect to LH. Ovulation should occur after about 36 to 48 hours, and so intercourse should be timed to coincide with this.
Intra-uterine insemination (IUI)
In around 20 per cent of infertility cases, there seems to be no problem with either partner. Surprisingly, in some of these cases, intra-uterine insemination proves successful. The basic idea behind IUI is to introduce the partner’s semen into the uterus.
The steps in IUI are as follows:
- Follicle development is stimulated and monitored.
- Treatment to induce ovulation is given.
- A fresh sperm sample is introduced into the uterus.
In vitro fertilisation (IVF)
A woman undergoing IVF treatment must endure weeks of hormone treatments, followed by the uncomfortable process of egg cell collection. Up to about 20 egg cells may be recovered. Her egg cells are fertilised by her partner’s sperm ‘in vitro’ and, when the tiny embryos have developed, two of these are put back into her uterus. IVF has, at best, about a 40 per cent success rate.
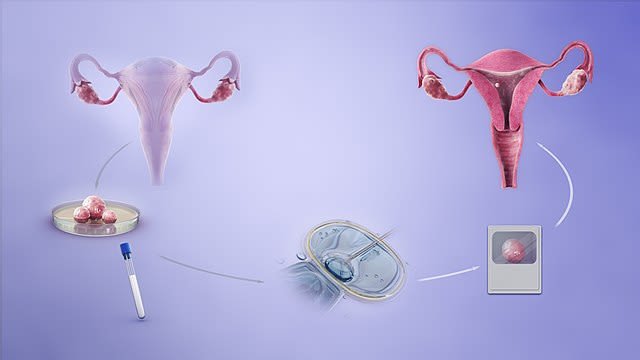
A depiction of the procedure of in-vitro fertilisation. http://www.scientificanimations.com, CC BY-SA 4.0
{kind=link}
‘in vitro’ (= in glass) fertilisation is what most people think of as ‘test-tube baby’ treatment. In IVF, the egg cells and sperm are taken from the couple and fertilised in a dish. The process of fertilisation normally takes 12 to 15 hours and after this the new embryos start to develop. Cell division is taken as a sign that fertilisation has been successful. Then, the tiny embryos (no more than balls of eight to 16 cells at this stage are placed into the uterus.
Gamete intra-Fallopian transfer (GIFT)
GIFT involves stimulating the ovaries and collecting the egg cells in much the same way as in IVF treatment. The important difference is that in GIFT the egg cells are mixed with sperm and immediately introduced into the Fallopian tubes, without waiting to see if fertilisation occurs. The advantage of this procedure – which would seem to be less controlled than IVF – is a 5 per cent better success rate. This is possibly because the Fallopian tube is the natural site for fertilisation: it may secrete chemicals that stimulate the process.
Ethical and moral considerations
Several aspects of IVF are very controversial. The procedure generates an excess of embryos that are never implanted, but they can be frozen and stored. Very early stage human embryos are an excellent source of stem cells for stem cell research and therapy. However, many people object to human embryos being used in this way. They argue that these balls of cells are living, potential human beings, and should never be used experimentally.
Another moral dilemma is whether IVF and other infertility treatments should be available on the NHS. The procedures are expensive and some people argue that the money would be better spent on cancer treatment, etc. They also point out that the human population is already spiralling out of control, and ask if using large amounts of medical resources to add to it is justified.
PREGNANCY, LABOUR AND BIRTH
In humans, pregnancy lasts for an average of 40 weeks. From around the twelfth week of pregnancy, progesterone secreted by the placenta inhibits uterine contractions. The level of progesterone rises steadily until just before birth, usually around 38 weeks after conception, when it starts to fall dramatically. This lifts the inhibition of uterine contractions, The mother’s anterior pituitary begins to secrete oxytocin and the placenta secretes prostaglandins, two hormones that actively promote contractions.
Oxytocin stimulates uterine contractions at about 40 weeks. The resulting tension in the muscle and pressure on the cervix are stimuli that bring about further secretion of oxytocin, causing more powerful contractions.
There are three stages of labour:
- Stage 1. The cervix dilates (opens) to a diameter of 10 cm.
- Stage 2. The fetus is pushed out of the uterus.
- Stage 3. The placenta and umbilical cord are expelled.

Stages in prenatal development. Mikael Häggström, Public Domain
{kind=link}
LACTATION
All mammals produce milk from specialized mammary glands. Humans are very special because they have permanent breasts which are made mainly of fatty tissue. The two main hormone in charge of producing milk are oestrogen and progesterone. Immediately after childbirth, the first fluid produced from the breasts is named colostrum. Colostrum has no fat but a very small amount of sugar which provides antibodies as a form of immunity to the newly born before it starts to produce its own immunity. In about thee to four days later, then the normal milk will be produced. And from then onwards, a constant supply of milk will commence. The stimulus of sucking at the nipple causes the posterior pituitary gland to secrete oxytocin. This hormone travels in the blood and causes contraction of the muscular myo-epithelial cells surrounding the milk glands or alveoli. This squeezes the milk out of the alveoli, through the milk ducts and into the infant’s mouth. This mechanism, called the let-down reflex, takes several seconds to take effect but is quite powerful. If the unsuspecting infant lets go of the nipple, it can get a jet of milk in the eye.
Throughout the period of lactation, the pituitary continues to secrete prolactin, a hormone that maintains the milk ducts and, to some extent, inhibits ovulation. This inhibition is called lactational anoestrus and reduces the risk of conception so soon after birth. However, it is not always effective and breast-feeding cannot be relied on as a contraceptive method.
SUMMARY
After reading this all my previous post on WHAT IS SEX FOR #1, #2, you should now be able to know and understand the following:
- Asexual reproduction usually involves one individual. All offspring are genetically identical: they are clones.
- Sexual reproduction involves two sexes which produce haploid gametes. Males produce spermatozoa by spermatogenesis, females make egg cells by oogenesis. Both processes involve a special type of cell division called meiosis.
- At fertilisation, a new diploid zygote is formed.
- The zygote, which is genetically unique, grows and develops by a series of mitotic divisions.
- The timing of reproductive events in humans is controlled by hormones. The hypothalamus controls the pituitary gland, which releases gonadotrophins. These stimulate the gonads to secrete steroids: oestrogen, progesterone and testosterone.
- The human menstrual cycle lasts, on average, for 28 days. The cycle begins with menstruation, which occurs as the next egg cell is prepared inside the ovary. By day 14 a new endometrium has grown. Ovulation takes place on day 14 and the egg cell is then available to be fertilised. If the egg cell is not fertilised, the endometrium breaks down and the cycle repeats.
- In humans, the egg cell is fertilised in the Fallopian tube. The zygote begins mitotic divisions becoming a morula and then a blastocyst as it moves along the tube towards the uterus. When the blastocyst has implanted in the endometrium, it is known as an embryo.
- The developing embryo (which is called a fetus after about 8 weeks) is nourished via the placenta, a temporary organ that does the job of the fetal lungs, intestines and excretory system.
- Birth is brought about by a series of hormonal changes that begin uterine contractions. In mammals, the infant is nourished by milk produced by the mother.
Thanks for coming.
REFERENCES
https://www.mayoclinic.org/healthy-lifestyle/pregnancy-week-by-week/in-depth/placenta/art-20044425
https://en.wikipedia.org/wiki/Placenta
https://www.webmd.com/infertility-and-reproduction/guide/understanding-infertility-treatment
https://www.medicalnewstoday.com/articles/165748.php
https://www.mayoclinic.org/diseases-conditions/infertility/diagnosis-treatment/drc-20354322
https://my.clevelandclinic.org/health/diseases/16083-infertility-causes
https://en.wikipedia.org/wiki/Ovulation_induction
https://www.uhcw.nhs.uk/ivf/treatments/oi/
https://americanpregnancy.org/getting-pregnant/intrauterine-insemination/
https://www.webmd.com/infertility-and-reproduction/guide/artificial-insemination
https://en.wikipedia.org/wiki/In_vitro_fertilisation
https://en.wikipedia.org/wiki/Gamete_intrafallopian_transfer
https://www.nhs.uk/conditions/pregnancy-and-baby/what-happens-during-labour-and-birth/
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.